The cruciate ligaments, the cranial and the caudal, of the stifle (knee) joint are cross shaped ligaments that connect the femur (thigh bone) to the tibia (shin bone). They are located within the stifle joint itself. The cranial cruciate ligament (CCL) is the most commonly injured cruciate ligament. Its role is to help maintain a normal relationship between the femur and the tibia in all angles of motion.
More specifically, the CCL prevents the tibia from sliding forward, relative to the femur. The cranial cruciate ligament also prevents excessive internal rotation of the tibia and plays a role in limiting hyperextension of the stifle (Figure 1).
Figure 1: Normal anatomy of the stifle.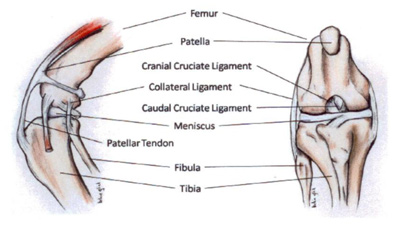
When the CCL ruptures or tears, the stifle becomes unstable and the normal relationship between the femur and the tibia is altered leading to inflammation (arthritis) and pain. If the instability is not treated, lameness persists and this leads to inflammation, and cartilage damage which will progress to osteoarthritis (OA). Because of the instability in the stifle caused by the ruptured cranial cruciate ligament, the medial meniscus can be pinched between the femur and the tibia causing irreparable damage. Subjectively, it appears that patients with CCL ruptures and meniscal damage are more painful (i.e. more lame) than patients without meniscal damage (Figure 2).
Figure 2: Instability of the stifle after cranial cruciate ligament rupture leads to inflammation, meniscal damage, pain and arthritis.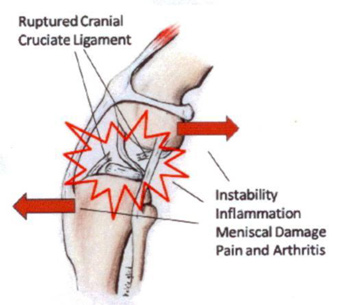
Incidence:
CCL rupture occurs much more frequently in dogs than cats. It is the most common orthopaedic injury of the hind limb in dogs in this practice and is the most common cause of degenerative joint disease in the stifle joint. CCL rupture occurs on dogs of all sizes but is more prevalent in large and giant breeds. Large breed dogs are more severely affected by the resulting instability. Typically it is a condition seen in middle aged overweight dogs, although it can be seen at any age.
Cause and Clinical Signs:
There is no single cause of CCL rupture. In most canine patients, there is a chronic deterioration of the cranial cruciate ligament that eventually leads to complete rupture and possible meniscal damage. This would suggest a conformational or possible immune-mediated issue. In the remaining patients, the tear is truly traumatic resulting from sudden, severe twisting or hyperextension of the stifle. The lameness often begins as a slight stiffness in the affected limb most notable after heavy exercise. The lameness typically progresses to the extent that the dog will refuse to use the affected limb. It is not uncommon for the cranial cruciate ligaments to deteriorate in both hind limbs simultaneously. Such patients compensate for this by shifting weight to their forelimbs. They assume a crouched stance and many people notice that their dogs are reluctant to climb stairs or jump into cars. The most common sign of CCL rupture is lameness in the affected hind limb. Any degree of lameness can be appreciated with this disorder depending on the completeness of the tear and the condition of the medial meniscus.
Diagnosis:
The diagnosis is usually made on physical examination. The stifle is manipulated to detect evidence of pain, swelling or instability. An anterior draw sign is diagnostic for a ruptured CCL.
Anaesthesia may be necessary to move the limb to the extent needed to make the diagnosis because pain from a ruptured CCL can be severe and muscle tension can restrict the motion of the joint. Radiographs (x-rays) are generally very helpful in making this diagnosis as they can demonstrate effusion (excessive fluid) in the joint as well as osteophytes (bone spurs) which both develop secondary to the arthritis. The ruptured ligament itself will not show up on radiographs. While the presence of effusion and bone spurs are not specific for CCL rupture, they are most commonly associated with CCL rupture and can support the physical examination findings. Arthroscopic evaluation of the stifle can also be performed to assess the joint in a minimally invasive manner. This allows a magnified view of the interior of the joint.
Treatment:
Non-surgical therapy does not address the biomechanical instability in the stifle. The goals of therapy are to relieve pain, restore function and minimize the rate of progression and ultimate extent of osteoarthritis by stabilizing the joint. Most patients are able to resume their preoperative life style. However, some patients will develop evidence of OA over time. The best results are obtained when surgery is performed to stabilise the joint and medical therapy is used to alleviate the signs associated with arthritis. Physical rehabilitation is beneficial in regaining muscle mass, muscle strength, and range of motion. There are numerous surgical techniques for the management of CCL rupture in our canine and feline patients. The most common techniques employed at the Greensborough Veterinary Hospital are the Tibial Tuberosity Advancement (TTA), used in dogs bigger than 20kg body weight and the LigaFiba Isotoggle generally used in cats and dogs less than 20kg body weight. Your pet is normally in hospital from 2 days to 6 days post operatively. We are happy to discuss these options and will work with you in determining the best treatment for your pet.
Home Care:
Regardless of which surgical option you decide upon, home care consists of strict confinement for a minimum of 4 to 6 weeks, giving all the prescribed medications and weekly visits to assess progress. This involves keeping your dog in a very small room or cage to limit movement, as excessive movement, or jumping in the first few weeks can lead to surgical procedures failing. In the following 4 to 5 months your dog can have restricted exercise like slow walks and only on a lead. After this time your pet should be back to 95% mobility, however muscular strength and development will take much longer to recover. It must be emphasised, that up to 40% of patients will rupture the cranial cruciate in the opposite stifle so care must be taken not to rush the rehabilitation process. It is an extremely important to monitor your pets weight, obesity can increase the risk of injury to the other knee as well as contributing to a more rapid rate of OA development. Your veterinarian will give you advice as to how things are progressing and guide you through the recovery process.
